In addition to taking the impression of the upper and lower arches, it is important to record the relationship between them in order to successfully create a positive model of accurate intercuspation.
To do this, we use bite registration, which is precisely the digital or analogue recording of how the two arches are positioned relative to one other. This is a crucial step, especially when dealing with prosthetics, orthodontics, and in general whenever analysing a patient’s occlusion, particularly if it is unstable. (1)
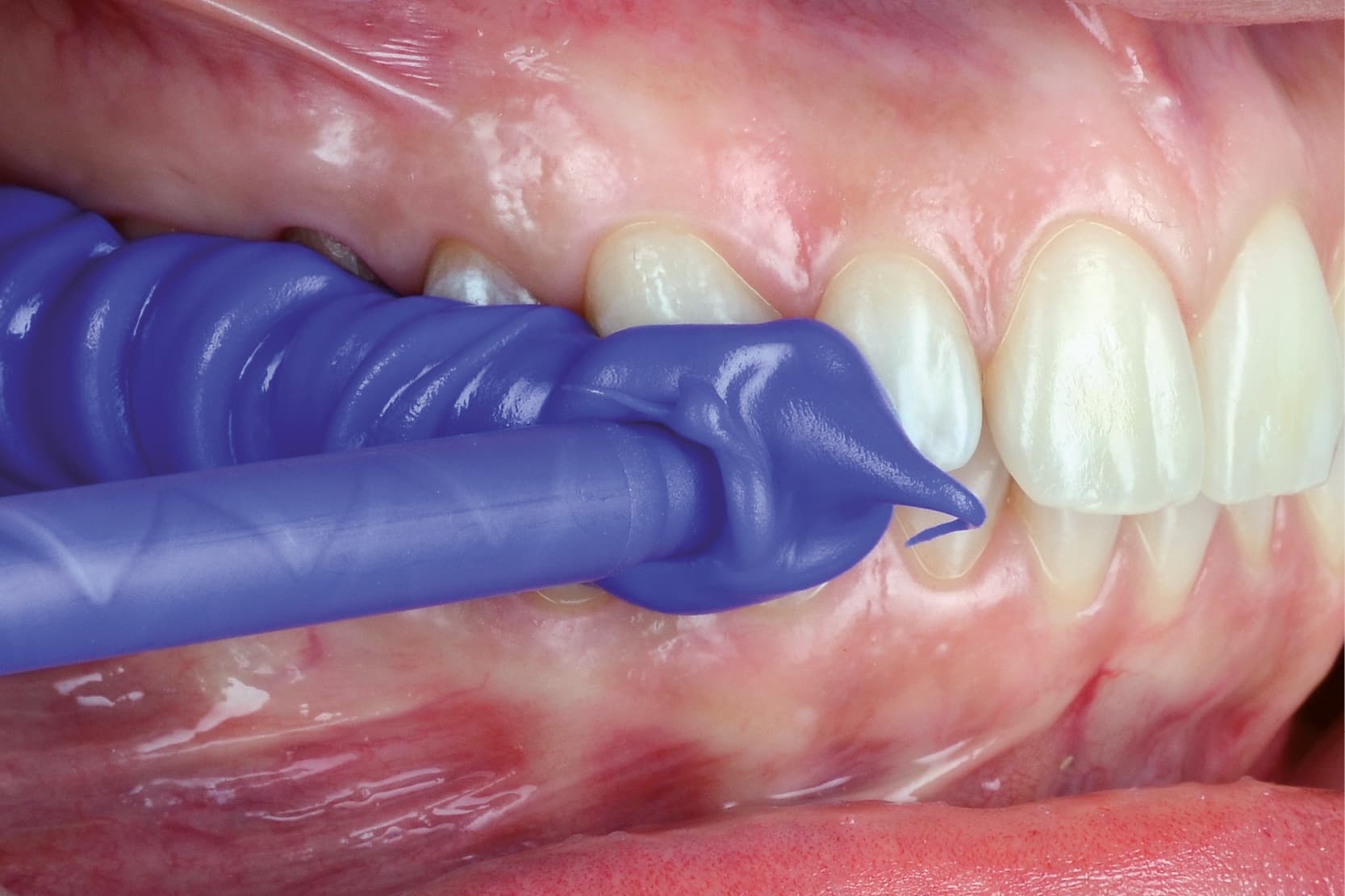
Traditionally, bite registration is performed by placing a material between the arches and asking the patient to clench their teeth in the position of interest that the clinician wants to record and/or analyse. The occlusion can be recorded at maximum intercuspation, centric relation or even with a possible elevation or advancement depending on the purpose of the procedure.
Digitally, however, after scanning the two arches, the patient is asked to close their mouth in the desired position and the occlusion is recorded sagittally and often bilaterally.
Analogue bite registration: advantages and limitations
The first materials used to perform an occlusal registration were natural waxes (3,4), but many others were developed later. (2)
Analogue bite registration can typically be performed using elastomers such as polyvinylsiloxanes (addition silicones), polyethers or materials such as waxes.
Although digital technologies are increasingly common, analogue bite registration still offers significant advantages in clinical practice. One of the main benefits is its accessibility and affordability.
Traditional materials such as waxes and silicones are widely available and relatively inexpensive (5). Analogue techniques are also well established and familiar to many clinicians, reducing the need for specific training and reliance on digital systems.
Analogue bite registrations can also be useful in complex prosthetic cases, where tactile feedback and visual inspection of the material help to accurately capture mandibular-maxillary relationships (6).
However, analogue bite registration also has some disadvantages. One of its main limitations is the inaccuracy resulting from deformation of the materials. Traditional materials such as waxes and silicones are subject to dimensional changes caused by temperature variations and improper handling, compromising accuracy (5).
Manual manipulation and patient movements during the procedure can also introduce errors, leading to incorrect articulation.
The process is also time consuming and labor intensive. Analogue methods require physical impressions, refinements and often repeat procedures, increasing chair time and reducing workflow efficiency (6). In addition, the storage and transportation of physical models represent a logistical challenge, risking further deterioration of the material.
The lack of real-time feedback is a further limitation of analogue methods, compared to digital systems, which instead allow for immediate analysis.
Digital bite registration: precision and innovation
Digital bite registration uses intraoral scanners to capture the spatial relationship between the maxillary and mandibular arches. The process involves scanning the vestibular surfaces while the patient is in maximum intercuspation, centric or functional occlusion. The collected data are converted into a digital 3D model, which can be analysed and transferred to CAD/CAM systems for diagnosis, planning and prosthetic manufacturing (7).
Digital technology offers numerous advantages over traditional analogue methods, particularly in terms of accuracy, efficiency and integration into digital workflows. One of its main benefits is its high precision, since digital scanners minimise errors related to material deformation and patient movements (7). At the same time, the process allows for real-time visualisation, permitting immediate analysis of occlusal relationships (8).
Digital registration reduces chair time and improves patient comfort, and the data acquired can be easily stored, duplicated and transmitted electronically, simplifying communication with dental laboratories and improving operational efficiency (9).
Despite its numerous advantages, however, digital bite registration also has some disadvantages. One of its main limitations is the high initial cost of intraoral scanners, which can be prohibitive for some dental practices (8). Furthermore, the steep learning curve and the need for adequate training may slow down integration and affect clinical efficiency during the transition phase (9).
Accuracy may also be compromised in several clinical situations, such as limited mouth opening or excessive salivation (7). Another factor that can complicate the workflow and lead to data loss is the need for compatibility between scanner software and CAD/CAM platforms.
In conclusion, bite registration represents a key step in many diagnostic and therapeutic processes in dentistry. In most applications, digital and traditional techniques are interchangeable, offering the same degree of accuracy and reliability. However, in certain complex situations, the clinician may still prefer an analogue technique.
- Paul, P., Banerjee, T. N., Banerjee, S., & Debnath, A. (2024). Evaluation of efficacy of digital or virtual bite registration over conventional techniques-A systematic review. Journal of Oral Biology and Craniofacial Research, 14(6), 785-792.
- Dwivedi, A., Maru, K., & Sharma, A. (2020). A comparative evaluation of three dimensional accuracy of different types of interocclusal recording materials-an in vitro study. Medicine and Pharmacy Reports, 93(3), 280.
- Michalakis KX, Pissiotis A, Anastasiadou V, Kapari D. An experimental study on particular physical properties of several interocclusal recording media. Part II: Linear Dimensional change and accompanying weight change. J Prosthodont. 2004;13:150-159.
- Anusavice K. Phillips’ science of dental materials. 11th ed., Saunders Publication, India; 2003. pp. 205-254.
- Abduo, J., & Lyons, K. (2012). Clinical considerations for increasing the dimensional accuracy of conventional bite registration materials. The Journal of Advanced Prosthodontics, 4(3), 130–136.
- da Costa, R. G., et al. (2010). The Journal of Prosthetic Dentistry, 103(1), 1–9.
- Mangano, F., Gandolfi, A., Luongo, G., & Logozzo, S. (2017). Intraoral scanners in dentistry: A review of the current literature. BMC Oral Health, 17(1), 149. https://doi.org/10.1186/s12903-017-0442-x
- Logozzo, S. et al. (2014). Optics and Lasers in Engineering, 54, 203–221.
- Rehmann, P., Thieken, R., & Wöstmann, B. (2016). Journal of Prosthetic Dentistry, 116(5), 643–649.
Would you like more information about Zhermack Dental products and solutions?
Contact us







